
 Blood pressure control and monitoring in UK pre- post-P4P
Blood pressure control and monitoring in UK pre- post-P4P The apparent lack of effectiveness of the pay for performance incentive strategy adopted by the U.K. among general practitioners should be cause for reflection among U.S. health care policymakers. While America begins its headlong rush into a number of variations on this theme, the results of the U.K. experience make it clear that, at best, monetary incentives should be viewed as adjunctive strategies for improving quality, NOT OUR MAIN OR ONLY STRATEGY. The results section from the abstract of the U.K. study (click here for link to full text of the paper published in BMJ, Jan ) is sobering;
Results: After accounting for secular trends, no changes in blood pressure monitoring (level change 0.85, 95% confidence interval −3.04 to 4.74, P=0.669 and trend change −0.01, −0.24 to 0.21, P=0.615), control (−1.19, −2.06 to 1.09, P=0.109 and −0.01, −0.06 to 0.03, P=0.569), or treatment intensity (0.67, −1.27 to 2.81, P=0.412 and 0.02, −0.23 to 0.19, P=0.706) were attributable to pay for performance. Pay for performance had no effect on the cumulative incidence of stroke, myocardial infarction, renal failure, heart failure, or all cause mortality in both treatment experienced and newly treated subgroups.
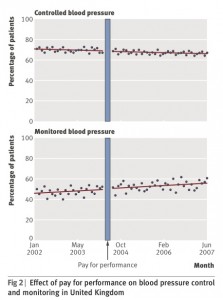
Example: Blood pressure monitoring rose modestly in line with trends present before pay for performance incentives (bottom chart of figure), but the percentage of patients with blood pressure controlled did not improve (top chart of figure). At best 70% of patients had their blood pressure under good control – or nearly 1/3 did not.
Why?: It is likely that most physicians intrinsically wish to take the best care of their patients that they can – so inherent motivation is already strong. [Deming - pride in workmanship] What we lack is a more effective system that enables better outcomes.
Conclusion: We need to redesign the whole system, rather than attribute all health outcomes to our primary care providers. What about interventions related to self-management coaching, health literacy, lifestyle behavior modification including nutrition, physical activity, etc.? The longer we delay designing reliable delivery models that address a broader range of effective preventive interventions, the sicker our system and our people will get. If we insist on focusing mainly on monetary incentives narrowly targeting our dedicated health care professionals, we set them and ourselves up for disappointing results. Money may intensify motivation (though perhaps less than expected among already committed health professionals), but by itself, does not provide the insight needed to improve the system. Applied research and development can.
Example: Blood pressure monitoring rose modestly in line with trends present before pay for performance incentives (bottom chart of figure), but the percentage of patients with blood pressure controlled did not improve (top chart of figure). At best 70% of patients had their blood pressure under good control – or nearly 1/3 did not.
Why?: It is likely that most physicians intrinsically wish to take the best care of their patients that they can – so inherent motivation is already strong. [Deming - pride in workmanship] What we lack is a more effective system that enables better outcomes.
Conclusion: We need to redesign the whole system, rather than attribute all health outcomes to our primary care providers. What about interventions related to self-management coaching, health literacy, lifestyle behavior modification including nutrition, physical activity, etc.? The longer we delay designing reliable delivery models that address a broader range of effective preventive interventions, the sicker our system and our people will get. If we insist on focusing mainly on monetary incentives narrowly targeting our dedicated health care professionals, we set them and ourselves up for disappointing results. Money may intensify motivation (though perhaps less than expected among already committed health professionals), but by itself, does not provide the insight needed to improve the system. Applied research and development can.