
Results
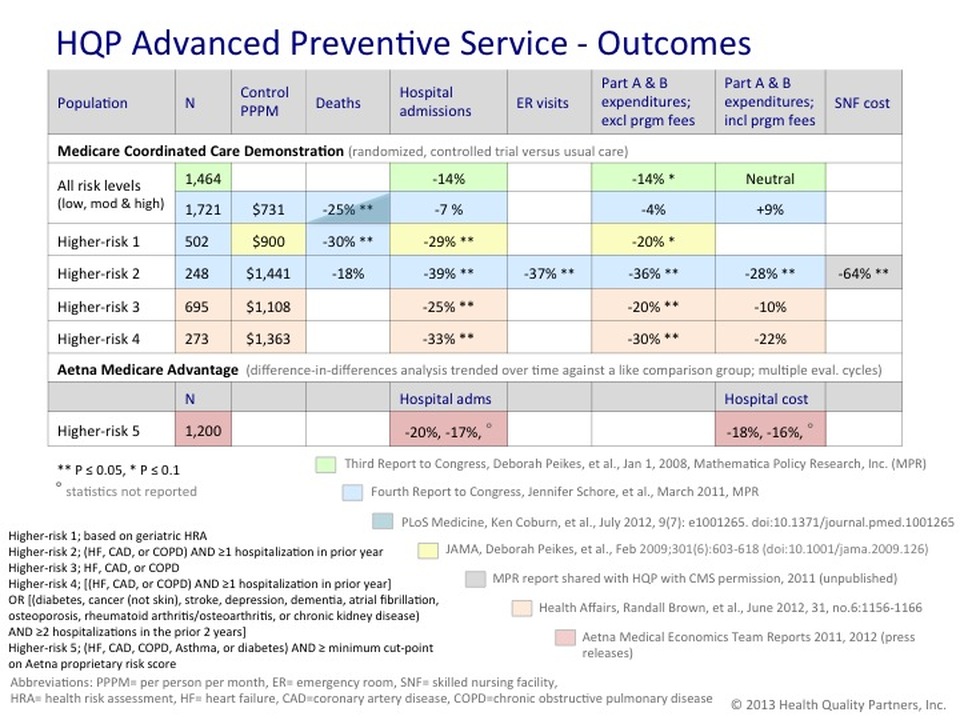
The evaluation of the HQP program has been the longest and most rigorous assessment of any care management model to date - more than 12 years. Within the Medicare Coordinated Care Demonstration (MCCD) the HQP program was tested in a randomized, controlled trial, analyzed on an intention to treat basis. Our program's primary aim of improving health outcomes among chronically ill older adults was clearly achieved and has been reported over multiple, independent evaluations over several years - a recent report finds a relative reduction in all-cause mortality of 34% at 2 years of enrollment (p=0.02) and 22% at 5 years (p=0.03) - with no known adverse events, side effects, or treatment-related complications. With regard to reducing net health care expenditures, appropriately selected higher-risk traditional Medicare (MCCD) and Medicare Advantage populations have had significant and durable reductions in hospitalizations (25-39%) and cost savings (10-28%). A detailed summary of the results of HQP's program among various subgroups and over the course of multiple analyses undertaken in evaluating our program is shown below.
In the final extension phase of the MCCD (2011-2014) several factors and conditions beyond HQP's control affected program implementation. HQP was required to use a revised eligibility criteria defined by ICD-9 codes and hospitalization, the practical implementation of which resulted in the enrollment of a significantly more costly and complex cohort than any of the 'higher-risk' subgroups previously identified and evaluated during the first 8 years of the demonstration. The latter cohort required a shift in the relative mix of services provided (e.g., fewer preventive health group programs, more home visits). Multiple operational disruptions due to the timing of key administrative decisions by CMS also substantially impaired the continuity and quality of service during the last extension phase. Finally, diminished statistical power due to small sample sizes and shorter average follow up times hampered the evaluation of this period of the demo.
When considered in the context of a significant program-related reduction in all-cause mortality, results achieved during the first 8 years of the demo, and the ongoing effectiveness of the HQP model in a Medicare Advantage population, analysis of the final phase of the MCCD may have limited utility except to serve as an important reminder that in order for programs delivering advanced preventive care to be effective, they must;
When considered in the context of a significant program-related reduction in all-cause mortality, results achieved during the first 8 years of the demo, and the ongoing effectiveness of the HQP model in a Medicare Advantage population, analysis of the final phase of the MCCD may have limited utility except to serve as an important reminder that in order for programs delivering advanced preventive care to be effective, they must;
- target populations that can most benefit from the intervention (both a broader definition of 'higher-risk' and participant motivation appears to be key)
- deliver a robust program having significant preventive care offerings with high reliability, and
- do so in a sustained, uninterrupted and cost effective manner